








Players Matters - July 2026
Players Matters
World Rugby Player Welfare Newsletter · July 2026
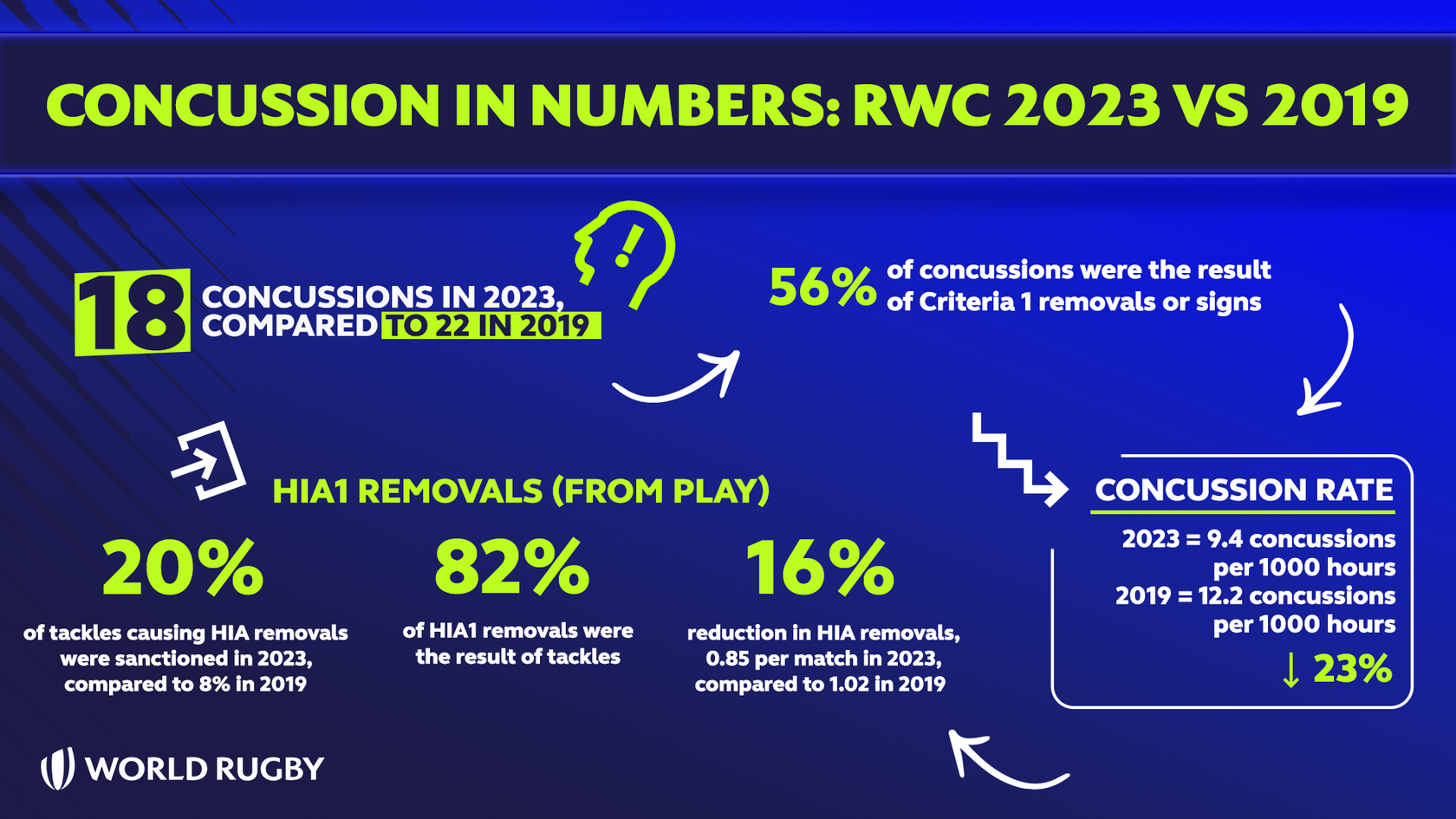
The 2025/26 SVNS season is done, and congratulations are due to South Africa’s men, who completed the Series and Championship double. In a season that split the women’s honours, New Zealand took the Series and Australia the Championship. Beyond the results, it was our biggest season yet for instrumented mouthguards (IMGs), and the data are beginning to tell a genuinely interesting story.
Instrumented mouthguards in SVNS: our largest cohort yet
Across nine tournaments, from Dubai in November to Bordeaux in June, we collated every head acceleration event (HAE) recorded by IMGs in the men’s and women’s series. Three themes stand out. The first is compliance. The proportion of each squad producing data averaged 60% in the men and 57% in the women, meaning around five players in every squad generated no data in a given match, and it declined both across the season and within each tournament. There were encouraging exceptions, with New Zealand’s men (71%) and Japan’s women (79%) showing what is routinely achievable. This is a solid start, but lifting compliance, and Day-2 and Day-3 wearing in particular, is the clear priority for the seasons ahead.
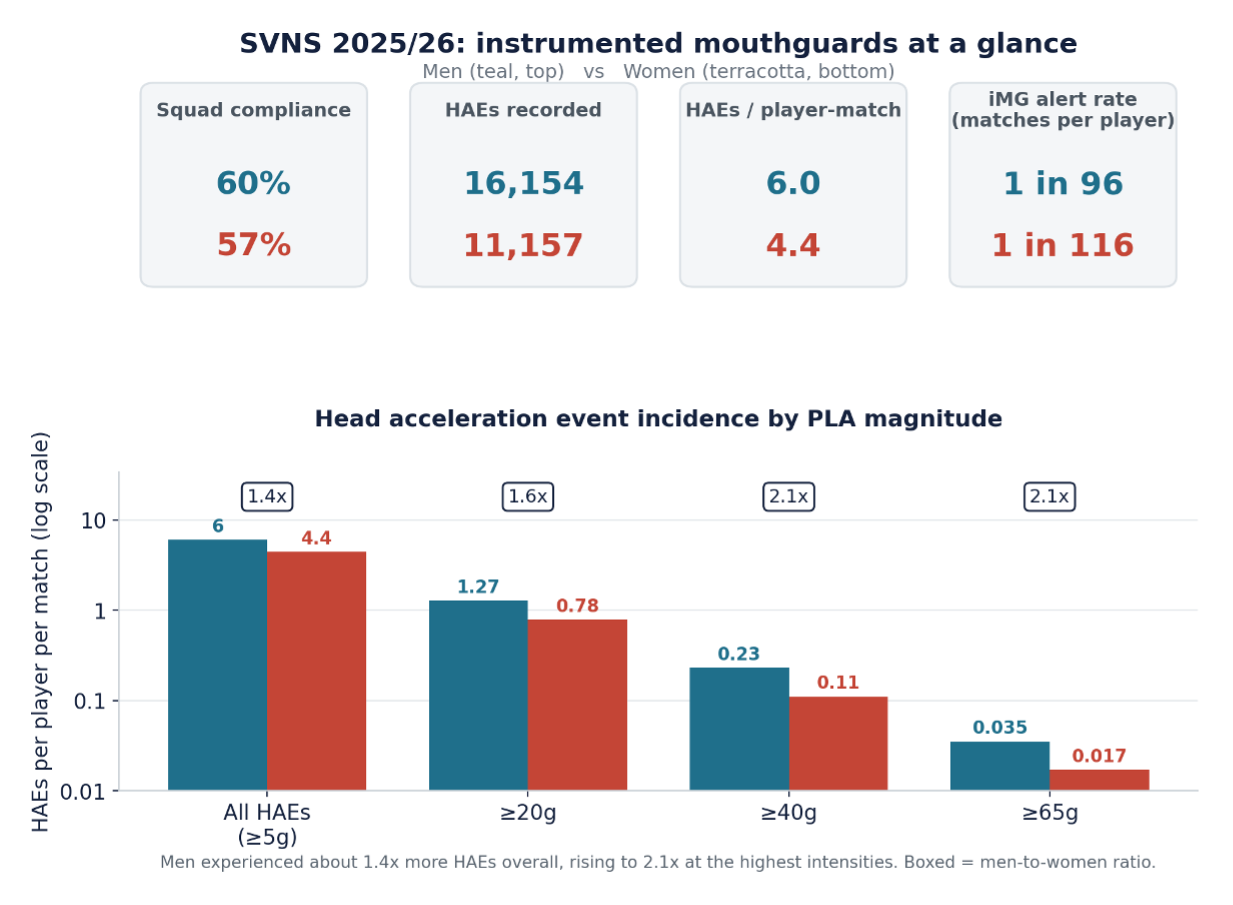
Figure 1. Men versus women: squad compliance, HAEs recorded, incidence and alert rate across the season.
The second theme is incidence. At every intensity, men experienced more head accelerations than women. The overall men’s rate was about 1.4 times higher than women’s (6.0 HAEs versus 4.4 HAEs per player per match), rising to 2.1-fold at 40g and above. This mirrors fifteens worldwide, and probably reflects differences in size, speed and thus kinetic energy during the contact events that cause the HAEs.
The much shorter matches in SVNS, combined with the three matches per day format, mean that at these rates, a SVNS player will experience about the same number of HAEs in a day of Sevens as in an 80-minute Fifteens match. Adjusted for the same period, SVNS HAEs occur at a higher rate than in Fifteens, as shown in Figure 2 below.
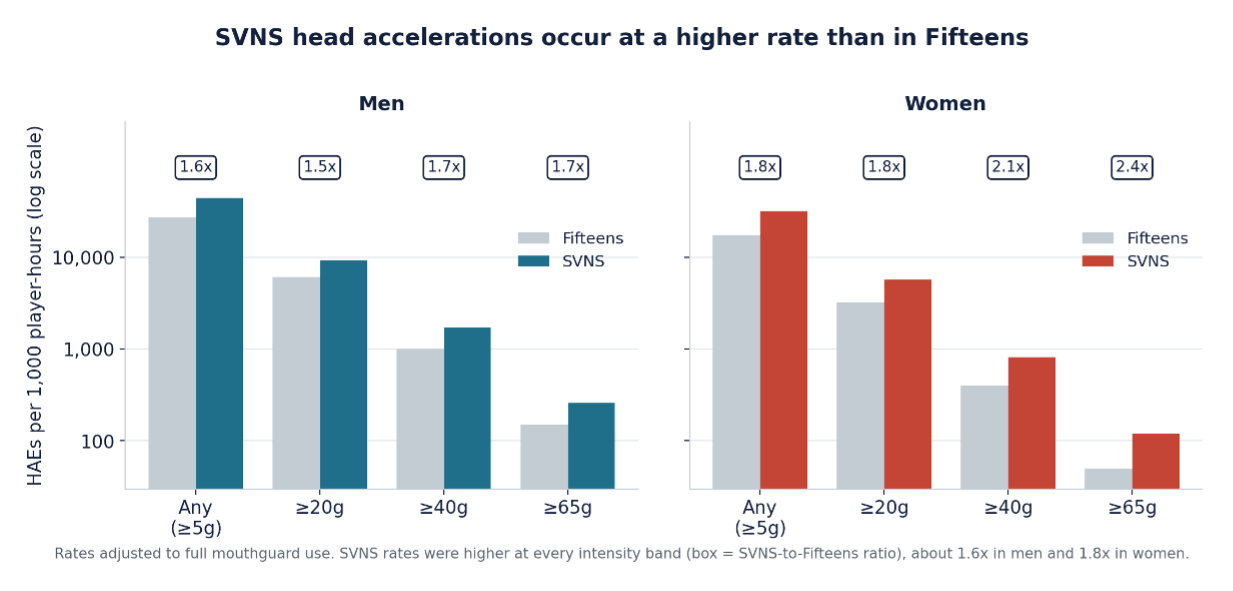
Figure 2. Head accelerations per 1,000 player-hours, SVNS versus Fifteens, adjusted to full mouthguard use.
The third theme, and perhaps the most important as we move forward with the IMG project, is that this load is not shared evenly. A small group of 10% of players accounted for approximately 30% of all recorded HAEs. These players can only be identified through the individual monitoring that the IMG provides, and so, much like has been described previously for Fifteens, we intend to develop the IMG system to monitor players and identify these higher HAE cases with a view to managing their cumulative exposure. IMG alerts, by contrast, remained rare, with more than 90% of team-matches passing without one. The present alert rate means that a typical player would experience an IMG alert removal every 96 matches (men) or 116 matches (women).
World Rugby lowers the community tackle height
Following a meeting in June, World Rugby has formally lowered the legal tackle height in the community game, confirming guidance first issued in 2023. The community game lacks the video review, officiating and daily coaching that changed elite behaviour through sanction, so law change is its best realistic lever. The decision rests on the largest dataset of its kind, more than 170,000 tackles coded across eleven Unions in a project delivered by World Rugby in partnership with the University of Cape Town.
The findings have been consistent and encouraging. The shape of the game was preserved, with tackle success, tackle counts and post-tackle play unchanged, while tacklers adopted safer positions. Upright tacklers fell from 36% to 29% in men, and from 51% to 44% in women.
Contact above the ball carrier’s sternum dropped from 42% to 38%. Where injury surveillance exists, the clinical data have been encouraging. France reported head and neck injury reductions of 54% for tacklers and 57% for ball carriers, with blue-card rates down 27%. Ireland’s injury surveillance showed a 52% concussion reduction in men and 20% in women, while in South Africa’s Varsity Cup, concussion declined 43%. No competition has reported an increase in concussions.
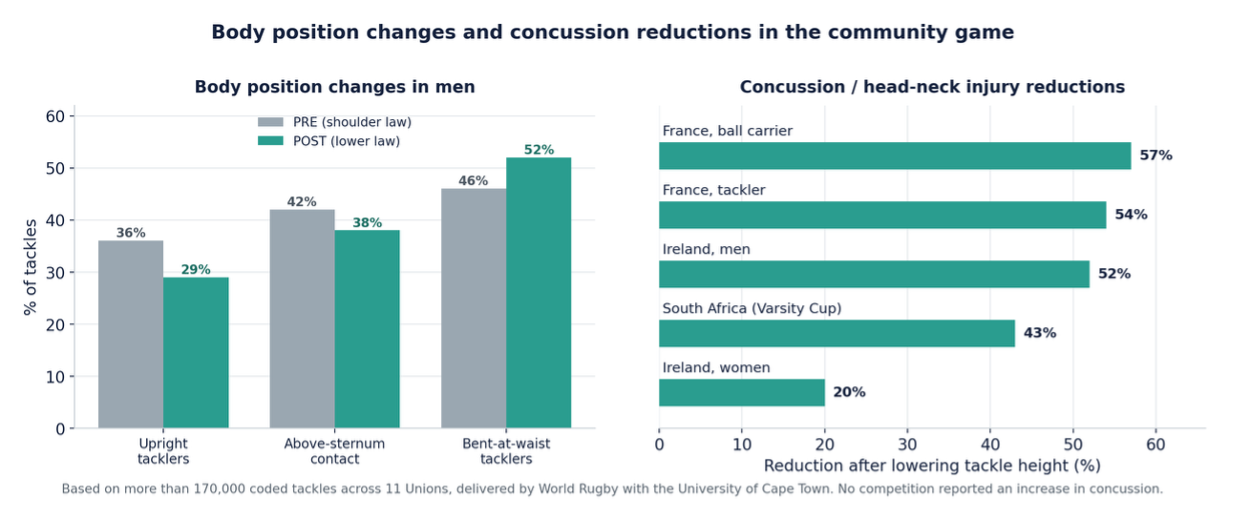
Figure 3. Community tackle height: safer tackler body position, and reduced concussion where surveillance exists.
South Africa did provide a very interesting counterexample, with South African junior women showing a reverse of the global trend, and more upright tacklers with lower height. We investigated this, and discovered that SARU had made a concerted effort to improve tackle technique the year before the lower height trial, but that this was not repeated in the year of the tackle height reduction. Our conclusion from this is that technique education makes a really significant impact on tackle technique, possibly more than law change, and it reminds us that law change alone should not be thought of as sufficient, and that coaching and technique development must be delivered as an integral part of the change, not an optional extra.
A first for the elite game: the U20 World Championship trial
While on the subject of tackle height, the 2026 U20 World Championship has just concluded, and with it the first elite trial in which we have lowered the tackle height in law, to the base of the sternum. The tournament was chosen deliberately. It is a closed competition with a three to four week preparation camp, and its players have largely come through age-grade rugby already playing under lower community heights. The trial was supported by secondary laws to manage the ball-carrier response, since when tacklers go lower, ball carriers tend to follow, and we must understand whether that relocates risk rather than removing it. My welfare team will now dedicate significant time to studying how the trial went, across six streams of analysis (see Figure 4). This analysis will be supported by feedback from player, coach and match-official surveys. Our aim is to inform future decisions with as much evidence as possible. The elite question is not closed, and it will be answered in time.

Figure 4. The six evaluation streams for the U20 lower-tackle-height trial.
Frankfurt meetings and the World Rugby Conference, October
Finally, some dates for the diary. The rugby science and welfare community gathers in Frankfurt at the end of October. The Rugby Science Network Meeting takes place on Sunday 25 October, World Rugby’s meetings and working groups convene on Monday 26 October, and the World Rugby Medical Conference follows on 27 and 28 October. Further detail, including the agenda, will be shared in due course, but we hope to see you all there in person.
|
Players’ Voice A new, standing section, contributed and owned by International Rugby Players. Working title; the name may evolve. This edition marks the start of something we are proud of. Over the last five years, our collaboration with the players, through International Rugby Players, has become closer and more candid than ever, and it is a partnership we value enormously. The players themselves have asked for a dedicated space in this newsletter to share their perspective on the welfare issues that matter to them, a request we welcomed without hesitation. Player welfare cannot be done to players; it has to be done with them, and giving them a standing voice here is a small but meaningful step towards that. My thanks to them for their engagement, and to all of you for your continued interest and contribution. With the introduction of more competitions to the global calendar, players are being asked to play more matches, which increase the amount of travel and training over the course of the year. In a milestone step for player load, World Rugby Executive Board endorsed five player load guidelines in October 2025. These guidelines were the work of World Rugby Player Load Group which involved staff, representatives from IRPA, professional competitions, unions and independent experts who are involved in the elite level of the game.
Details regarding these recommendations can be found here: https://www.world.rugby/news/1017767/world-rugby-executive-board-agrees-new-player-load-guidelines. The challenge with developing these guidelines is the lack of data from the global game with the majority of data that informed the development of these guidelines being drawn from the England PREM competition. In response IRPA, supported by World Rugby, set up a global study to examine player load across a full year in the following elite level competitions in the men’s game: · Super Rugby Pacific · Japan Rugby Leasure Div 1 · Premiership Rugby · Top 14 · United Rugby Championship. The aim of this study is to understand how much physical, mental and life-load players experience across a full year of elite rugby and the impact this has on their health and wellbeing. We have completed the first domestic competition as part of Phase 1 with four Super Rugby Teams and 2 Japan Rugby League Div 1 and will continue to follow players through the international window and any additional domestic competitions. We are in preparation for the start of the Northern Hemisphere and South African Pre-season and are working with teams to kick Phase 2 of the project off. In addition, we also hope to work with Premiership Women’s Rugby, which will enable us to have the first look at developing women’s specific guidelines.
|
